The World Health Organization recommends exclusive breastfeeding (EBF) for the first six months of life as the gold standard for infant nutrition and a low-cost strategy to reduce infant mortality. This has proven to have been effective when fully adhered to in both developing and developed countries. The major challenge among nursing mothers especially in developing countries is the issue of compliance as recommended by World Health Organization. Among the several factors contributing to full compliance of EBF, socio-cultural factors play a significant role. This cross-sectional descriptive survey examined sociocultural factors influencing EBF among 360 nursing mothers attending immunization clinics at primary health centers in Ado Local Government Area, Ado-Ekiti, Ekiti State. Using a multi-stage sampling technique and an interviewer-administered questionnaire, data were collected on socioeconomic and demographic characteristics and sociocultural influences and analyzed with SPSS version 25. Findings showed that 78 (21.7%) respondents believed boys should be exclusively breastfed, 250 (69.4%) believed their breasts would sag after EBF, and 88 (24.4%) reported that mother-in-laws or traditional birth attendants could make them give herbal preparations to their babies before six months. These results indicate that the child’s sex, education level, family/spousal support, misconceptions about colostrum and breast milk adequacy, and community practices (such as herbal use) are important sociocultural determinants of EBF in this setting.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Breastfeeding is how nutrition is provided for the healthy growth and development of infants by putting the nipple of the mother’s breast into the mouth of the baby
[1]
Ike MN (2013) Utilization of exclusive breastfeeding methods among nursing mothers in Nigeria. Mediterr J Soc Sci 4(8): 69
.It is also an integral part of the reproductive process, with important implications for maternal health. Breastfeeding contributes to the health and well-being of mothers, helps to space children, reduces the risk of ovarian and breast cancers, and increases family and natural resources
[1]
Ike MN (2013) Utilization of exclusive breastfeeding methods among nursing mothers in Nigeria. Mediterr J Soc Sci 4(8): 69
. It is a secure way of feeding infants and is safe for both mother and child. The balance of nutrients and chemical constituents in breast milk from a healthy mother makes it ideal for young infants
[2]
World Health Organization (n.d.) Exclusive breastfeeding for optimal growth, development and health of infants. WHO eLENA.
. The American Association of Pediatrics (AAP) defines exclusive breastfeeding as an infant's consumption of human milk with no supplementation of any type (no water, no juice, no non-human milk, and no foods), except for vitamins, minerals, and medications. EBF for the first six months of life is estimated to lower infant deaths by 13%
[3]
Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, Bellagio Child Survival Study Group (2003) How many child deaths can we prevent this year? Lancet 362(9377): 65-71
Several factors determine mothers' knowledge, attitudes, and practices regarding breastfeeding, particularly exclusive breastfeeding. These determinants differ from place to place. Studies in Peninsular Malaysia have indicated that rural residence, ethnicity, non-working and non-smoking mothers, multiparous mothers, term infants, mothers with husbands who support breastfeeding, and mothers who practice bed-sharing are positively associated with exclusive breastfeeding
[4]
Uganda Bureau of Statistics (2002-2003) Uganda population and housing census 2002-2003: main report. Uganda Bureau of Statistics, Kampala.
[4]
.
In a longitudinal cohort study in the Canadian province of Nova Scotia, among mothers who initiated breastfeeding, significant predictors of early cessation of exclusive breastfeeding were less than high school education, lowest neighborhood income quintile, single motherhood, pregnancy, obesity, smoking throughout pregnancy, no early breast contact by the infant (<1 hour after birth), and no intention to breastfeed
[5]
Aarts C, Kylberg E, Hörnell A, Hofvander Y, Gebre‑Medhin M, Greiner T (2000) How exclusive is exclusive breastfeeding? A comparison of data since birth with current status data. Int J Epidemiol 29(6): 1041-1046.
A study that investigated why mothers stop breastfeeding in the United States stated that the top three reasons for mothers stopping breastfeeding within the first month and between the first and second month after their child’s birth include “Baby had trouble sucking and latching on” (53.7% and 27.1%, respectively), “Breast milk alone didn’t satisfy my baby” (49.7% and 55.6%), and “I didn’t have enough milk” (51.7% and 52.2%)
[6]
Bland RM, Rollins NC, Coutsoudis A, Coovadia HM, Child Health Group (2002) Breastfeeding practices in an area of high HIV prevalence in rural South Africa. Acta Paediatr 91(6): 704-711.
Factors associated with suboptimal breastfeeding and feeding practices in Nairobi, Kenya, include child’s sex, perceived size at birth, mother’s marital status, ethnicity, education level, family planning (pregnancy desirability), health-seeking behavior (place of delivery), and neighborhood (slum of residence)
[7]
Kimani‑Murage EW, Madise NJ, Fotso JC, Kyobutungi C, Mutua MK, Gitau TM, Yatich N (2011) Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health 11: 396.
. A study conducted in Bahirdar city, Ethiopia, showed that independent predictors for exclusive breastfeeding practice were mothers’ education, child sex, parity, family size, and time of postnatal care in this study area
[8]
Smith MM, Kuhn L (2000) Exclusive breast‑feeding: does it have the potential to reduce breast‑feeding transmission of HIV‑1? Nutr Rev 58(11): 333-340.
A national study conducted by Tedros Alemayehu et al. depicted exclusive breastfeeding prevalence at 49.0% and independently associated with maternal education, marital status, wealth index, and child age
[9]
Alemayehu T, Haidar J, Habte D (2009) Determinants of exclusive breastfeeding practice in Ethiopia. Ethiop J Health Dev 23.
. This study assessed the sociocultural factors influencing exclusive breastfeeding of infants among nursing mothers attending Primary Health Care centers in Ado-Ekiti, Ekiti State.
2. Methodology
The study was conducted in Ado-Ekiti, the state capital and headquarters of Ekiti State, in the southwestern part of Nigeria. Geographically, Ado Ekiti in the Ado local government is located at latitude 700 40' North of the Equator and longitude 500 16' east of the Greenwich Meridian
[10]
Ekiti State Government (n.d.) Ado‑Ekiti Local Government Area. Ekiti State Government, Ado‑Ekiti.
. Ado-Ekiti Local Government is a one-town local government that also serves as the Local Government and State headquarters, which is approximately 200m above sea level in the southeastern part of the Ireje stream and 500m above sea level in the northeastern limit
[10]
Ekiti State Government (n.d.) Ado‑Ekiti Local Government Area. Ekiti State Government, Ado‑Ekiti.
The people of Ado-Ekiti are mostly of the sub-ethnic group of Yoruba, while Hausas, Ebiras, Igbos, and other ethnic groups are residents in clusters, especially in the suburbs of Ado-Ekiti. The Federal Government has divided the Ado Local Government into 13 political wards
[10]
Ekiti State Government (n.d.) Ado‑Ekiti Local Government Area. Ekiti State Government, Ado‑Ekiti.
. The predominant occupations of this population of interest are farming, trading, civil service, teaching, lecturing, and office work.
There are five tertiary institutions and one Technical College in the local government, namely Ekiti State University, Federal Polytechnic, School of Nursing, Crown Polytechnic, and Afe Babalola University. Several secondary institutions, federal and state ministries, and private establishments that provide a wide range of job opportunities for various categories of vibrant workers are also located within the local government
[10]
Ekiti State Government (n.d.) Ado‑Ekiti Local Government Area. Ekiti State Government, Ado‑Ekiti.
. In Ekiti State, there are three public tertiary health facilities, 19 public secondary health facilities, and 325 public primary health facilities. There are 45 primary health facilities in Ado LGA. Of these, 32 are public and 13 are private primary health facilities
[11]
Ado O (n.d.) Facility type ownership code. (Unpublished/grey source).
[11]
.
The study design was cross-sectional and descriptive, with the study population being women with children between 0 days and 24 months of age attending the immunization clinic and mothers after delivery at the hospital.
The minimum sample size was determined using Fisher’s formula, and a sample size of 360 was determined. The sample size (n) for a population greater than 10,000 was determined using Fisher’s formula. Where:
(1)
The minimum sample size (nf) for a population of less than 10,000 was determined using Cochran’s (1977) formula for finite population
[12]
Bartlett JE, Kotrlik JW, Higgins CC (2001) Organizational research: determining appropriate sample size in survey research. Inf Technol Learn Perform J 19(1): 43-50.
[12]
.
(2)
n = desired sample size (when the population is greater than 10,000)
Z = standard normal deviate at 95% confidence level = 1.96 from the normal distribution table
d = desired precision = 5% = 0.05 (degree of accuracy required)
p = prevalence of EBF = 52.6% (prevalence and predictors of exclusive breastfeeding among mothers in a semi-urban Nigerian community: a cross-sectional study
[13]
Adebayo AM, et al. (2021) Prevalence and predictors of exclusive breastfeeding among mothers in a semi‑urban Nigerian community: a cross‑sectional study. Ann Ib Postgrad Med 2021 Jun; 19(1): 31-39.
[13]
= 0.526
q = 1-p (proportion of the target population not having the characteristics)
nf = is the sample size for a population less than 10,000
N which is the estimated study population size is taken to be 2000.
With 10% response rate as 32.13, the total sample size is 353.39, approximately the nearest ten to be 360. An introductory letter was obtained from the Department of Community Medicine, Ekiti State University Teaching Hospital, and delivered to the Ekiti State Primary Health Development Agency requesting permission to conduct the study. The respondents were recruited using a multi-stage sampling technique (three stages, random sampling by balloting). The instrument of study was a pretested semi-structured questionnaire covering the socio-demographic data of respondents and the socio-cultural factors influencing EBF, which was revised as needed and subsequently administered to the study population. Participation in the study was voluntary, including nursing mothers with children aged 0 days to 23 months attending immunization clinics in PHCs in Ado LGA. Data was analyzed using the International Business Machine (IBM) Statistical Package for Social Science (SPSS) version 25.
3. Results
Table 1 displays the age group, ethnicity, education, occupation, religion, marital status, number of children, mode of delivery, and average monthly income of respondents.
Table 1. Socio-economic and Demographic Characteristics of Respondents.
Variables
N= 360 Frequency (n)
Percentage (%)
Age
10 - 19
10
2.8
20 - 29
161
44.7
30 - 39
178
49.4
40 - 49
11
3.1
Ethnicity
Yoruba
331
91.9
Igbo
8
2.2
Hausa
6
1.7
Others
15
4.2
Education
Primary
60
16.7
Secondary
105
29.2
Tertiary
195
54.2
Occupation
Trading
222
61.7
Teaching
61
16.9
Civil Servant
4
1.1
Student
3
0.8
Hairdressing
20
5.6
Tailoring
30
8.3
Others
20
5.6
Religion
Christianity
157
43.6
Muslim
141
39.2
Others
62
17.2
Marital Status
Single
1
0.3
Married
359
99.7
No. Of Children
1
65
18.1
2
116
32.2
3
127
35.3
Others
52
14.4
Delivery Mode
Vaginal Delivery
248
68.9
Caesarean Section
112
31.1
Average Family Income
Less than ₦33,000
164
45.6
₦33,000 - ₦50,000
120
33.3
Greater than ₦50,000
76
21.1
Most respondents were between 20 and 39 years of age. Most of the study respondents were Yoruba (91.9%), and 54% had a tertiary level of education. Furthermore, most respondents were traders (61.7%), and 99.7% were married. The most common mode of delivery among respondents was vaginal delivery (68.9%).
Table 2 shows the frequency of assessment of respondents' socio-cultural factors as they affect exclusive breastfeeding.
Table 2. Socio - Cultural Factors among Study Respondents.
Variables
Frequency (Percentage%)
Yes
No
Boys should Exclusively Breastfeed than Girls
78 (21.7)
282 (78.3)
Breasts Sagging after Exclusive Breastfeeding
110 (30.6)
250 (69.4)
Colostrum is Dirty or a Taboo
1 (0.3)
359 (99.7)
Breastfeeding Babies in Public Spaces
344 (95.6)
16 (4.4)
Giving Babies other foods before Exclusive Breastfeeding
0 (0.0)
360 (100)
Family Supports Exclusive Breastfeeding
357 (99.2)
3 (0.8)
Husband Supports Exclusive Breastfeeding
353 (98.1)
7 (1.9)
Forced to give Babies herbs before they are 6 months old by Mother in-law and Traditional attendants
88 (24.4)
272 (75.6)
Not Enough Breast Milk for your Baby
103 (28.6)
257 (71.4)
Stay for days before Breastfeeding Baby after Birth
64 (17.8)
296 (82.2)
In this study, 282 (78.3%) of the respondents did not think that boys should be breastfed exclusively and 250 (69.4%) of the respondents thought that their breasts would sag after exclusive breastfeeding. In addition, 359 (99.7%) of the respondents did not believe that colostrum was dirty or taboo, and 344 (95.6%) of the respondents stated that breastfeeding babies in public places was a good attitude. In addition, 360 (100.0%) respondents did not believe that babies should be given other foods before exclusive breastfeeding. Most respondents 357 (99.2%) reported that their families supported exclusive breastfeeding. In this study, 353 (98.1%) respondents stated that their husbands supported exclusive breastfeeding. A few respondents 88 (24.4%) also stated that they could be made to give herbs to their babies before they are 6 months old by their mother-in-law and traditional birth attendants. In addition, 103 (28.6%) of the respondents stated that they did not have enough breast milk for their babies. Most of the respondents, 296 (82.2%) did not have to stay days before breastfeeding their babies.
Table 3. Association Between the Socio-Economic and Demographic Characteristics of Study Respondents and Socio-Cultural Factors of EBF.
Socio-Cultural Factors among Respondents Affecting EBF.
Good Socio-Cultural Factors n (%)
Poor Socio-Cultural Factors n (%)
Statistics
p-value
Age
43.36
<0.0001
10 - 19
4 (40)
6 (60.0)
20 - 29
152 (94.4)
9 (5.6)
30 - 39
167 (93.8)
11 (6.2)
40 - 49
11 (100.0)
0 (0.0)
Ethnicity
Yoruba
308 (93.1)
23 (6.9)
1.18
0.76
Igbo
7 (87.5)
1 (12.5)
Hausa
5 (83.3)
1 (16.7)
Others
14 (93.3)
1 (6.7)
Level of Education
Primary
56 (93.3)
4 (6.7)
0.05
0.977
Secondary
97 (92.4)
8 (7.6)
Tertiary
181 (92.8)
14 (7.2)
Occupation
Trader
212 (95.5)
10 (4.5)
24.63
<0.0001
Teacher
49 (80.3)
12 (19.7)
Civil Servant
3 (75.0)
1 (25.0)
Student
2 (66.7)
1 (33.3)
Hairdressing
20 (100.0)
0 (0.0)
Tailoring
28 (93.3)
2 (6.7)
Others
20 (100.0)
0 (0.0)
Religion
Christian
132 (84.1)
25 (15.9)
31.49
<0.0001
Muslim
140 (99.3)
1 (0.7)
Others
62 (100.0)
0 (0.0)
Marital Status
Single
1 (100.0)
0 (0.0)
0.08
0.78
Married
333 (55.9)
26 (44.1)
Divorce
0 (0.0)
0 (0.0)
Number of Children
1
60 (92.3)
5 (7.7)
4.24
0.24
2
108 (93.1)
8 (6.9)
3
121 (95.3)
6 (4.7)
>/= 4
45 (86.5)
7 (13.5)
Mode of Delivery
Vaginal delivery
236 (95.2)
12 (4.8)
6.76
0.009
Caesarean section
98 (87.5)
14 (12.5)
Average Family Income
<33,000.00
162 (98.8)
2 (1.2)
25.23
<0.0001
33,000.00 - 50,000.00
100 (83.3)
20 (16.7)
>50,000.00
72 (94.7)
4 (5.3)
Table 3 above shows the association between the demographic characteristics of the respondents and socio-cultural factors of exclusive breastfeeding. The result shows that most of our respondents between the ages 30-39, 167 (93.8%) had good socio-cultural factors of exclusive breastfeeding, and most of the respondents who are Traders, 212 (95.5%) had good socio-cultural factors of exclusive breastfeeding, also Among the responders, the majority who were Christians, 132 (84.1%) had good socio-cultural factors of exclusive breastfeeding. The majority who had a vaginal delivery, 236 (95.2%) had good socio-cultural factors of exclusive breastfeeding, and most respondents with an average income of <#33, 000, 157 (95.7%) had good socio-cultural factors of exclusive breastfeeding. It was revealed in the study that there was a significant association between the socio-economic and demographic characteristics - age, occupation, religion, mode of delivery, and average family income - of respondents with a 5% level of significance.
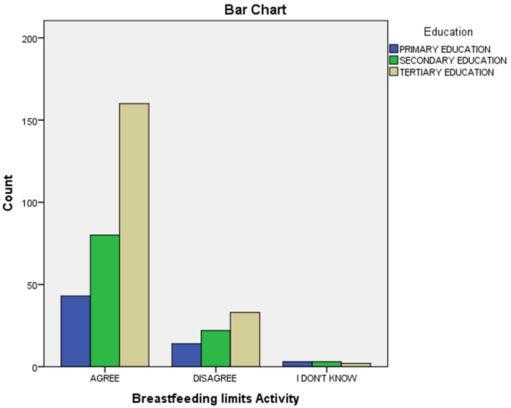
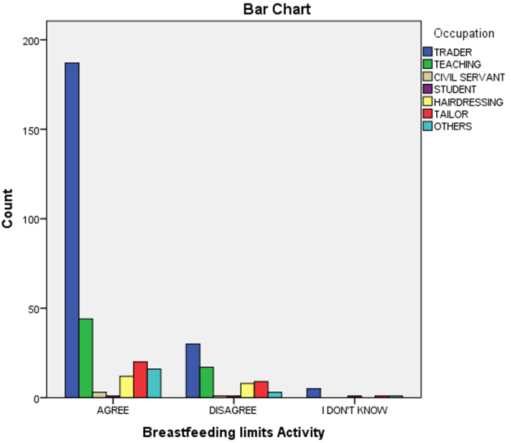
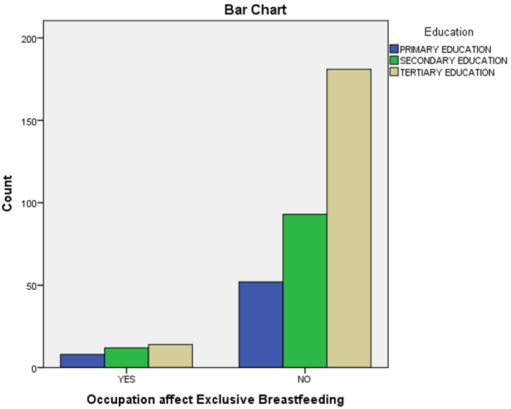
Figure 3. Respondents’ reactions to EBF were affected by occupation filtered with relation to their Level of Education.
4. Discussion
This study determined the socio-cultural factors influencing EBF among nursing mothers attending immunization clinics in the Ado Local Government Area (LGA). Three hundred and sixty respondents were recruited for the study. The findings of this study showed the socio-cultural factors affecting mothers’ exclusive breastfeeding. In this study, the majority (78.3%) of the respondents did not think that boys should be breastfed exclusively compared to girls. This is in contrast to the results of previous studies conducted in East Africa, where cultural beliefs mentioned that "Baby boy" need solid foods immediately because they make them strong and healthy, and if a child is breastfed on breast milk alone for six months, the bones get weak
[14]
Tadele N, Habta F, Akmel D, et al. (2016) Knowledge, attitude and practice towards exclusive breastfeeding among lactating mothers in Mizan Aman town, Southwestern Ethiopia: descriptive cross‑sectional study. Int Breastfeed J 11: 3.
. From the study, more than two-thirds (69.4%) of respondents thought their breasts would sag after exclusive breastfeeding. This agrees with a similar study conducted in Adamawa, Nigeria, where 60% of nursing mothers agreed that EBF flattens the breast
[15]
Tyndall JA, Kamai R, Chanchangi D (2018) Knowledge, attitudes and practices on exclusive breastfeeding in Adamawa, Nigeria. Am J Public Health Res 4(3): 112-119.
Findings from this study revealed that nearly all (99.7%) of respondents did not believe that colostrum is dirty or taboo. This agrees with a study carried out in Amasiri LGA, Ebonyi State, where 81.1% of nursing mothers believed that colostrum was good for the baby
[16]
Amadi E (n.d.) Knowledge, attitude and practice of exclusive breastfeeding among nursing mothers in Amasiri, Afikpo North Local Government Area, Ebonyi State, Nigeria. MOUAU Repository.
https://afribary.org/work/view/knowledge-attitude-and-practice-of-exclusive-breastfeeding-among-nursing- mothers- in-amasiri-afikpo-north-local-government-area-ebonyi-state-nigeria-amadi-esther-7-2
[16]
. From this study, more than nine-tenths (95.6%) of the respondents stated that breastfeeding babies in public places is good practice. This agrees with a similar study conducted in Suva, Fiji, where most nursing mothers (86.8%) agreed that women should breastfeed in public places
[17]
Temoirokomalani MD, Singh P, Khan S (2021) Knowledge, attitude and practices of breastfeeding among mothers of children under 6 months of age in Suva, Fiji. Curr Res Nutr Food Sci J 9(3): 1000-1016
. All (100.0%) respondents did not give any other foods before exclusive breastfeeding. This aligns with the result of a study conducted in a tertiary care center in Aurangabad, India, where most of the respondents (about 89%) did not give pre-lacteal feeds before EBF
[18]
Deshmukh V, Rasool U, Kalyankar B, Gaikwad R, Yelikar K (2016) Knowledge, attitude and practice of breastfeeding at a tertiary care centre in the government medical college and hospital, Aurangabad, India. Int J Reprod Contracept Obstet Gynecol 5(6): 1912-1915.
Most respondents (99.2%) reported that their families supported exclusive breastfeeding. This corroborates a similar study carried out in Juba, South-sudan, where 86.7% of nursing mothers affirmed that their family members supported breastfeeding
[19]
Warille EB. Knowledge and Practice of Exclusive Breastfeeding among Women with Children between 9 and 12 months of age in El Sabbah Hospital Juba South Sudan. 2015
. Nearly all (98.1%) respondents stated that their husbands supported exclusive breastfeeding. This is supported by the results of a study conducted in an infant welfare clinic in Osogbo, Osun State, where 93.3% of mothers had spousal support
[20]
Odu S, Deji SA, Amu E, Aduayi V (2016) Knowledge, attitude and practice of exclusive breastfeeding among mothers attending an infant welfare clinic in Osogbo, Osun State, Nigeria. Eur J Prev Med 4(2): 39-43.
. Less than one-third (24.4%) of respondents also stated that they could be made to give herbs to their babies before 6 months by their mother-in-law and traditional birth attendants. However, in a similar study in an infant welfare clinic in Osogbo, Osun State, Nigeria, 21.3% of the respondents claimed that they gave herbs or concoctions during EBF, and 73.8% thought herbs should be added while practicing EBF in the same study
[20]
Odu S, Deji SA, Amu E, Aduayi V (2016) Knowledge, attitude and practice of exclusive breastfeeding among mothers attending an infant welfare clinic in Osogbo, Osun State, Nigeria. Eur J Prev Med 4(2): 39-43.
Less than one-third (28.6%) of the respondents stated that they did not have enough breast milk for their babies. This did not corroborate the results of the systematic review conducted in East Africa, where 52.4% of the respondents believed that EBF was not enough for the baby in the first 6 months.
[21]
Dukuzumuremyi, J.P.C., Acheampong, K., Abesig, J. et al. Knowledge, attitude, and practice of exclusive breastfeeding among mothers in East Africa: a systematic review. Int Breastfeed J 15, 70 (2020).
In a similar study conducted in Boditi, Southern Ethiopia, 53.2% claimed that breast milk was not enough for the baby
[13]
Adebayo AM, et al. (2021) Prevalence and predictors of exclusive breastfeeding among mothers in a semi‑urban Nigerian community: a cross‑sectional study. Ann Ib Postgrad Med 2021 Jun; 19(1): 31-39.
[13]
. From the study, about four in five respondents (82.2%) did not have to stay for days before breastfeeding their babies. This is not in agreement with the report of a study carried out in Somalia, where most children are put to breast 2 - 3days after delivery and colostrum is not fed to the children by most of the mothers as it is considered heavy, thick, coarse, dirty, toxic, and harmful to children’s health
[22]
Somali Knowledge Attitude and Practices Study (KAPS) (n.d.) Infant and young child feeding and health seeking practices - Somalia. ReliefWeb.
Furthermore, the significant associations in Table 3 between socio-demographic characteristics and socio-cultural factors of exclusive breastfeeding (EBF) highlight multiple influences on breastfeeding practices in Ado Local Government Area. The findings revealed that older mothers aged 30-39 years showed greater support for EBF (93.8%), which may be attributed to accumulated maternal experience and better understanding, helping to counter myths such as breast sagging after breastfeeding. This result aligns with a tertiary care hospital study where maternal age was identified as a key predictor of EBF
[23]
Chineke HN, et al. (2017) The practice of exclusive breastfeeding and its sociodemographic determinants amongst nursing mothers at a tertiary health care institution in South East, Nigeria. Open J Prev Med 7(4): 63-73.
. Occupation also influenced breastfeeding attitudes. Most traders (95.5%) demonstrated favorable socio-cultural factors supporting EBF compared to 80.3% of teachers, likely reflecting flexible work schedules which enable continued breastfeeding despite cultural challenges. Similar occupational differences in EBF have been reported in Ekiti State
[24]
Owoeye S (2021) Factors affecting exclusive breastfeeding among nursing mothers in Ekiti State, Nigeria. World J Innov Res 10(2).
Moreover, religion was significantly associated with EBF perceptions. Most Muslim (99.3%) and other faith respondents (100%) showed positive attitudes toward EBF, surpassing Christians (84.1%), possibly due to religious teachings emphasizing natural infant feeding. Regarding mode of delivery, vaginal delivery mothers (95.2%) showed stronger EBF support than those who underwent cesarean sections (87.5%), consistent with Nigerian studies reporting delayed lactation and breastfeeding challenges following caesarean section
[25]
Onah S, Osuorah DIC, Ebenebe J, Ezechukwu C, Ekwochi U, Ndukwu I (2014) Infant feeding practices and maternal socio‑demographic factors that influence practice of exclusive breastfeeding among mothers in Nnewi South‑East Nigeria: a cross‑sectional and analytical study. Int Breastfeed J 9(1): 6.
. Unexpectedly, family income showed that the lowest earners (<₦33,000) had the highest proportion (98.8%) of good socio-cultural EBF factors, suggesting that limited financial resources might encourage reliance on breastfeeding rather than costly alternatives. Family support for exclusive breastfeeding was overwhelmingly strong, with 99.2% of respondents reporting family encouragement, corroborating studies in Juba, South Sudan
[19]
Warille EB. Knowledge and Practice of Exclusive Breastfeeding among Women with Children between 9 and 12 months of age in El Sabbah Hospital Juba South Sudan. 2015
. Spousal support was similarly high at 98.1%, consistent with findings from Osogbo, Osun State. Despite this, 24.4% of mothers reported pressure from in-laws or traditional birth attendants to give herbs to their babies before six months, echoing similar findings in Osogbo
[20]
Odu S, Deji SA, Amu E, Aduayi V (2016) Knowledge, attitude and practice of exclusive breastfeeding among mothers attending an infant welfare clinic in Osogbo, Osun State, Nigeria. Eur J Prev Med 4(2): 39-43.
. Concerning milk supply, 28.6% perceived their breast milk as insufficient, contrasting with higher rates reported in East Africa where over half of mothers shared this belief
[21]
Dukuzumuremyi, J.P.C., Acheampong, K., Abesig, J. et al. Knowledge, attitude, and practice of exclusive breastfeeding among mothers in East Africa: a systematic review. Int Breastfeed J 15, 70 (2020).
. Lastly, public breastfeeding received strong acceptance (95.6%), signaling a positive cultural shift. However, unlike some African regions with male-infant feeding bias, only 21.7% of mothers believed boys should receive preferential EBF, further reflecting community-specific cultural beliefs
[21]
Dukuzumuremyi, J.P.C., Acheampong, K., Abesig, J. et al. Knowledge, attitude, and practice of exclusive breastfeeding among mothers in East Africa: a systematic review. Int Breastfeed J 15, 70 (2020).
This study highlights the interplay of socio-cultural and economic factors shaping exclusive breastfeeding behaviors in Ado LGA. Effective interventions should target younger mothers, dispel myths about breast sagging and milk sufficiency. Community programs should build on family support by involving grandmothers and husbands, as recommended in northwest Nigeria research
[26]
Joseph FI, Earland J (2019) A qualitative exploration of the sociocultural determinants of exclusive breastfeeding practices among rural mothers, North West Nigeria. Int Breastfeed J 14(1): 38.
. Embedding these programs in Ekiti’s primary health centers is crucial to sustaining improvements in maternal and child health outcomes.
5. Conclusion
In conclusion, this study revealed several important sociocultural factors that influence exclusive breastfeeding practices among nursing mothers in Ado Local Government Area. While most mothers did not believe colostrum was taboo or that other foods should be given before 6 months, misconceptions persisted about breast sagging and gender differences in breastfeeding needs. Family support, especially from husbands, was crucial for successful exclusive breastfeeding. However, pressure from mothers-in-law and traditional birth attendants to give herbal concoctions remained a challenge for some mothers. Socioeconomic factors like education level, occupation, and income also played a role. Overall, the findings highlight the need for targeted education and support to address cultural beliefs and enable more mothers to exclusively breastfeed for the recommended 6 months. Ongoing monitoring of sociocultural influences, extended maternity leave, workplace accommodations, and early breastfeeding education could help improve exclusive breastfeeding rates in this community.
6. Recommendation
A comprehensive, ongoing survey of socio-cultural factors influencing exclusive breastfeeding (EBF) should be implemented to address the limitations of this cross-sectional study. This longitudinal approach would provide valuable insights into the dynamic population of nursing mothers and capture evolving trends over time. Additionally, expanding the research to include other local governments and rural areas within the state would offer a more comprehensive understanding of EBF prevalence and predictors across diverse settings.
To support EBF practices, it is recommended that maternity leave be extended to approximately six months. This extension would enable nursing mothers to exclusively breastfeed their infants without the challenges associated with balancing work commitments and breastfeeding. Furthermore, introducing breastfeeding education into school curricula would be beneficial in educating young people of both genders about the importance of EBF, preparing them as future parents. This early intervention could potentially lead to increased awareness and adoption of EBF practices in the long term.
Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, Bellagio Child Survival Study Group (2003) How many child deaths can we prevent this year? Lancet 362(9377): 65-71
Uganda Bureau of Statistics (2002-2003) Uganda population and housing census 2002-2003: main report. Uganda Bureau of Statistics, Kampala.
[5]
Aarts C, Kylberg E, Hörnell A, Hofvander Y, Gebre‑Medhin M, Greiner T (2000) How exclusive is exclusive breastfeeding? A comparison of data since birth with current status data. Int J Epidemiol 29(6): 1041-1046.
Bland RM, Rollins NC, Coutsoudis A, Coovadia HM, Child Health Group (2002) Breastfeeding practices in an area of high HIV prevalence in rural South Africa. Acta Paediatr 91(6): 704-711.
Kimani‑Murage EW, Madise NJ, Fotso JC, Kyobutungi C, Mutua MK, Gitau TM, Yatich N (2011) Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health 11: 396.
Ado O (n.d.) Facility type ownership code. (Unpublished/grey source).
[12]
Bartlett JE, Kotrlik JW, Higgins CC (2001) Organizational research: determining appropriate sample size in survey research. Inf Technol Learn Perform J 19(1): 43-50.
[13]
Adebayo AM, et al. (2021) Prevalence and predictors of exclusive breastfeeding among mothers in a semi‑urban Nigerian community: a cross‑sectional study. Ann Ib Postgrad Med 2021 Jun; 19(1): 31-39.
[14]
Tadele N, Habta F, Akmel D, et al. (2016) Knowledge, attitude and practice towards exclusive breastfeeding among lactating mothers in Mizan Aman town, Southwestern Ethiopia: descriptive cross‑sectional study. Int Breastfeed J 11: 3.
Tyndall JA, Kamai R, Chanchangi D (2018) Knowledge, attitudes and practices on exclusive breastfeeding in Adamawa, Nigeria. Am J Public Health Res 4(3): 112-119.
Amadi E (n.d.) Knowledge, attitude and practice of exclusive breastfeeding among nursing mothers in Amasiri, Afikpo North Local Government Area, Ebonyi State, Nigeria. MOUAU Repository.
https://afribary.org/work/view/knowledge-attitude-and-practice-of-exclusive-breastfeeding-among-nursing- mothers- in-amasiri-afikpo-north-local-government-area-ebonyi-state-nigeria-amadi-esther-7-2
[17]
Temoirokomalani MD, Singh P, Khan S (2021) Knowledge, attitude and practices of breastfeeding among mothers of children under 6 months of age in Suva, Fiji. Curr Res Nutr Food Sci J 9(3): 1000-1016
Deshmukh V, Rasool U, Kalyankar B, Gaikwad R, Yelikar K (2016) Knowledge, attitude and practice of breastfeeding at a tertiary care centre in the government medical college and hospital, Aurangabad, India. Int J Reprod Contracept Obstet Gynecol 5(6): 1912-1915.
Warille EB. Knowledge and Practice of Exclusive Breastfeeding among Women with Children between 9 and 12 months of age in El Sabbah Hospital Juba South Sudan. 2015
Odu S, Deji SA, Amu E, Aduayi V (2016) Knowledge, attitude and practice of exclusive breastfeeding among mothers attending an infant welfare clinic in Osogbo, Osun State, Nigeria. Eur J Prev Med 4(2): 39-43.
Dukuzumuremyi, J.P.C., Acheampong, K., Abesig, J. et al. Knowledge, attitude, and practice of exclusive breastfeeding among mothers in East Africa: a systematic review. Int Breastfeed J 15, 70 (2020).
Chineke HN, et al. (2017) The practice of exclusive breastfeeding and its sociodemographic determinants amongst nursing mothers at a tertiary health care institution in South East, Nigeria. Open J Prev Med 7(4): 63-73.
Onah S, Osuorah DIC, Ebenebe J, Ezechukwu C, Ekwochi U, Ndukwu I (2014) Infant feeding practices and maternal socio‑demographic factors that influence practice of exclusive breastfeeding among mothers in Nnewi South‑East Nigeria: a cross‑sectional and analytical study. Int Breastfeed J 9(1): 6.
Joseph FI, Earland J (2019) A qualitative exploration of the sociocultural determinants of exclusive breastfeeding practices among rural mothers, North West Nigeria. Int Breastfeed J 14(1): 38.
Deji, S. A., Folayan, T. A., Bakare, O. O., Falade, O. O., Awoyemi, O. R., et al. (2026). Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. European Journal of Preventive Medicine, 14(4), 59-69. https://doi.org/10.11648/j.ejpm.20261404.11
Deji, S. A.; Folayan, T. A.; Bakare, O. O.; Falade, O. O.; Awoyemi, O. R., et al. Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. Eur. J. Prev. Med.2026, 14(4), 59-69. doi: 10.11648/j.ejpm.20261404.11
Deji SA, Folayan TA, Bakare OO, Falade OO, Awoyemi OR, et al. Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. Eur J Prev Med. 2026;14(4):59-69. doi: 10.11648/j.ejpm.20261404.11
@article{10.11648/j.ejpm.20261404.11,
author = {Samson Ayo Deji and Temiloluwa Adeola Folayan and Olaoluwa Olumide Bakare and Oluwadunsin Ololade Falade and Oluwatosin Roseline Awoyemi and Tolulope Oluwabunmi Famewo and Damilola Dorcas Babalola and Olabisi Catherine Adekamimo and Ayomide Oluwagbenga Ayilola},
title = {Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria},
journal = {European Journal of Preventive Medicine},
volume = {14},
number = {4},
pages = {59-69},
doi = {10.11648/j.ejpm.20261404.11},
url = {https://doi.org/10.11648/j.ejpm.20261404.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20261404.11},
abstract = {The World Health Organization recommends exclusive breastfeeding (EBF) for the first six months of life as the gold standard for infant nutrition and a low-cost strategy to reduce infant mortality. This has proven to have been effective when fully adhered to in both developing and developed countries. The major challenge among nursing mothers especially in developing countries is the issue of compliance as recommended by World Health Organization. Among the several factors contributing to full compliance of EBF, socio-cultural factors play a significant role. This cross-sectional descriptive survey examined sociocultural factors influencing EBF among 360 nursing mothers attending immunization clinics at primary health centers in Ado Local Government Area, Ado-Ekiti, Ekiti State. Using a multi-stage sampling technique and an interviewer-administered questionnaire, data were collected on socioeconomic and demographic characteristics and sociocultural influences and analyzed with SPSS version 25. Findings showed that 78 (21.7%) respondents believed boys should be exclusively breastfed, 250 (69.4%) believed their breasts would sag after EBF, and 88 (24.4%) reported that mother-in-laws or traditional birth attendants could make them give herbal preparations to their babies before six months. These results indicate that the child’s sex, education level, family/spousal support, misconceptions about colostrum and breast milk adequacy, and community practices (such as herbal use) are important sociocultural determinants of EBF in this setting.},
year = {2026}
}
TY - JOUR
T1 - Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria
AU - Samson Ayo Deji
AU - Temiloluwa Adeola Folayan
AU - Olaoluwa Olumide Bakare
AU - Oluwadunsin Ololade Falade
AU - Oluwatosin Roseline Awoyemi
AU - Tolulope Oluwabunmi Famewo
AU - Damilola Dorcas Babalola
AU - Olabisi Catherine Adekamimo
AU - Ayomide Oluwagbenga Ayilola
Y1 - 2026/07/11
PY - 2026
N1 - https://doi.org/10.11648/j.ejpm.20261404.11
DO - 10.11648/j.ejpm.20261404.11
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 59
EP - 69
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20261404.11
AB - The World Health Organization recommends exclusive breastfeeding (EBF) for the first six months of life as the gold standard for infant nutrition and a low-cost strategy to reduce infant mortality. This has proven to have been effective when fully adhered to in both developing and developed countries. The major challenge among nursing mothers especially in developing countries is the issue of compliance as recommended by World Health Organization. Among the several factors contributing to full compliance of EBF, socio-cultural factors play a significant role. This cross-sectional descriptive survey examined sociocultural factors influencing EBF among 360 nursing mothers attending immunization clinics at primary health centers in Ado Local Government Area, Ado-Ekiti, Ekiti State. Using a multi-stage sampling technique and an interviewer-administered questionnaire, data were collected on socioeconomic and demographic characteristics and sociocultural influences and analyzed with SPSS version 25. Findings showed that 78 (21.7%) respondents believed boys should be exclusively breastfed, 250 (69.4%) believed their breasts would sag after EBF, and 88 (24.4%) reported that mother-in-laws or traditional birth attendants could make them give herbal preparations to their babies before six months. These results indicate that the child’s sex, education level, family/spousal support, misconceptions about colostrum and breast milk adequacy, and community practices (such as herbal use) are important sociocultural determinants of EBF in this setting.
VL - 14
IS - 4
ER -
Deji, S. A., Folayan, T. A., Bakare, O. O., Falade, O. O., Awoyemi, O. R., et al. (2026). Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. European Journal of Preventive Medicine, 14(4), 59-69. https://doi.org/10.11648/j.ejpm.20261404.11
Deji, S. A.; Folayan, T. A.; Bakare, O. O.; Falade, O. O.; Awoyemi, O. R., et al. Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. Eur. J. Prev. Med.2026, 14(4), 59-69. doi: 10.11648/j.ejpm.20261404.11
Deji SA, Folayan TA, Bakare OO, Falade OO, Awoyemi OR, et al. Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria. Eur J Prev Med. 2026;14(4):59-69. doi: 10.11648/j.ejpm.20261404.11
@article{10.11648/j.ejpm.20261404.11,
author = {Samson Ayo Deji and Temiloluwa Adeola Folayan and Olaoluwa Olumide Bakare and Oluwadunsin Ololade Falade and Oluwatosin Roseline Awoyemi and Tolulope Oluwabunmi Famewo and Damilola Dorcas Babalola and Olabisi Catherine Adekamimo and Ayomide Oluwagbenga Ayilola},
title = {Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria},
journal = {European Journal of Preventive Medicine},
volume = {14},
number = {4},
pages = {59-69},
doi = {10.11648/j.ejpm.20261404.11},
url = {https://doi.org/10.11648/j.ejpm.20261404.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20261404.11},
abstract = {The World Health Organization recommends exclusive breastfeeding (EBF) for the first six months of life as the gold standard for infant nutrition and a low-cost strategy to reduce infant mortality. This has proven to have been effective when fully adhered to in both developing and developed countries. The major challenge among nursing mothers especially in developing countries is the issue of compliance as recommended by World Health Organization. Among the several factors contributing to full compliance of EBF, socio-cultural factors play a significant role. This cross-sectional descriptive survey examined sociocultural factors influencing EBF among 360 nursing mothers attending immunization clinics at primary health centers in Ado Local Government Area, Ado-Ekiti, Ekiti State. Using a multi-stage sampling technique and an interviewer-administered questionnaire, data were collected on socioeconomic and demographic characteristics and sociocultural influences and analyzed with SPSS version 25. Findings showed that 78 (21.7%) respondents believed boys should be exclusively breastfed, 250 (69.4%) believed their breasts would sag after EBF, and 88 (24.4%) reported that mother-in-laws or traditional birth attendants could make them give herbal preparations to their babies before six months. These results indicate that the child’s sex, education level, family/spousal support, misconceptions about colostrum and breast milk adequacy, and community practices (such as herbal use) are important sociocultural determinants of EBF in this setting.},
year = {2026}
}
TY - JOUR
T1 - Socio-cultural Factors Influencing Exclusive Breastfeeding Among Nursing Mothers Attending Primary Health Care Centers in Nigeria
AU - Samson Ayo Deji
AU - Temiloluwa Adeola Folayan
AU - Olaoluwa Olumide Bakare
AU - Oluwadunsin Ololade Falade
AU - Oluwatosin Roseline Awoyemi
AU - Tolulope Oluwabunmi Famewo
AU - Damilola Dorcas Babalola
AU - Olabisi Catherine Adekamimo
AU - Ayomide Oluwagbenga Ayilola
Y1 - 2026/07/11
PY - 2026
N1 - https://doi.org/10.11648/j.ejpm.20261404.11
DO - 10.11648/j.ejpm.20261404.11
T2 - European Journal of Preventive Medicine
JF - European Journal of Preventive Medicine
JO - European Journal of Preventive Medicine
SP - 59
EP - 69
PB - Science Publishing Group
SN - 2330-8230
UR - https://doi.org/10.11648/j.ejpm.20261404.11
AB - The World Health Organization recommends exclusive breastfeeding (EBF) for the first six months of life as the gold standard for infant nutrition and a low-cost strategy to reduce infant mortality. This has proven to have been effective when fully adhered to in both developing and developed countries. The major challenge among nursing mothers especially in developing countries is the issue of compliance as recommended by World Health Organization. Among the several factors contributing to full compliance of EBF, socio-cultural factors play a significant role. This cross-sectional descriptive survey examined sociocultural factors influencing EBF among 360 nursing mothers attending immunization clinics at primary health centers in Ado Local Government Area, Ado-Ekiti, Ekiti State. Using a multi-stage sampling technique and an interviewer-administered questionnaire, data were collected on socioeconomic and demographic characteristics and sociocultural influences and analyzed with SPSS version 25. Findings showed that 78 (21.7%) respondents believed boys should be exclusively breastfed, 250 (69.4%) believed their breasts would sag after EBF, and 88 (24.4%) reported that mother-in-laws or traditional birth attendants could make them give herbal preparations to their babies before six months. These results indicate that the child’s sex, education level, family/spousal support, misconceptions about colostrum and breast milk adequacy, and community practices (such as herbal use) are important sociocultural determinants of EBF in this setting.
VL - 14
IS - 4
ER -