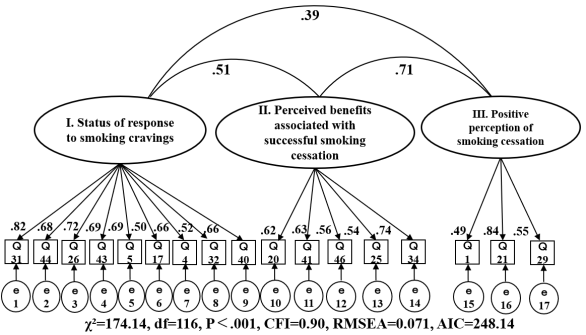
The purpose of this study was to develop and test the reliability and validity of a scale assessing the efforts made by midlife adult male smokers to quit smoking. The draft of the scale, designated the Smoking Cessation Assessment of Progress Scale (SCAPS), was developed a qualitative inductive analysis of the characteristics of successful smoking cessation efforts among midlife adult male workers in a previous study by the authors. The subjects were men in their 30s and 40s who were employed, had quit smoking for at least six months, and who had succeeded in quitting without seeking outpatient smoking cessation treatment. After a preliminary survey, the main survey was conducted. Data was analyzed using the maximum likelihood Promax rotation method. Confirmatory factor analysis was subsequently conducted, resulting in the identification of three factors and 17 items. The factors identified were "response to smoking cravings," "perceived benefits associated with successful smoking cessation," and "positive perception of smoking cessation. Cronbach's alpha coefficients for each subscale ranged from 0.702 to 0.873, which were generally favorable. Construct validity was generally ensured by confirmatory factor analysis and the estimates extracted from the results for each factor. The reliability and validity of SCAPS were generally verified.
| Published in | European Journal of Preventive Medicine (Volume 12, Issue 2) |
| DOI | 10.11648/j.ejpm.20241202.13 |
| Page(s) | 47-62 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Middle-Aged, Males, Worker, Quit Smoking Support, Scale, Smoking Cessation
(n=105) | |||
|---|---|---|---|
n | % | ||
Age | |||
30s | 38 | (36.2) | |
40s | 67 | (63.8) | |
Employment category | |||
Construction | 4 | (4.8) | |
Manufacturing | 32 | (30.5) | |
Electricity, gas, heat supply, and water supply | 2 | (1.9) | |
Information communications industry | 1 | (1.0) | |
Transportation and postal services | 9 | (8.6) | |
Wholesale and retail | 1 | (1.0) | |
Finance and insurance | 1 | (1.0) | |
Education and learning support | 2 | (1.9) | |
Service industry | 2 | (1.9) | |
Civil service and government | 50 | (47.6) | |
Unknown | 1 | (1.0) | |
Number of Employees | |||
Less than 100 | 14 | (13.3) | |
More than 100 but less than 300 | 23 | (21.9) | |
More than 300 but less than 1,000 | 33 | (31.4) | |
More than 1,000 | 34 | (32.4) | |
Unknown | 1 | (1.0) | |
Job type | |||
Managerial | 13 | (12.4) | |
Professional and technical | 17 | (16.2) | |
Clerical | 50 | (47.6) | |
Sales | 2 | (1.9) | |
Service | 1 | (1.0) | |
Production | 15 | (14.3) | |
Transportation and driving | 5 | (4.8) | |
Unknown | 2 | (1.9) | |
Employment status | |||
Regular employee | 105 | (100.0) | |
Temporary staff and contract employees | 0 | 0.0 | |
Marital status | |||
Married | 93 | (88.6) | |
Unmarried | 12 | (11.4) | |
Highest level of education | |||
High school | 43 | (41.0) | |
Vocational school | 8 | (7.6) | |
University | 53 | (50.5) | |
Graduate school | 1 | (1.0) | |
Age when commencing smoking | |||
Under 15 years old | 2 | (1.9) | |
15 to 18 years old | 13 | (12.4) | |
18 to 21 years old | 75 | (71.4) | |
21 to 24 years old | 5 | (4.8) | |
24 years old or older | 10 | (9.9) | |
Average number of cigarettes smoked per day | |||
Less than 10 | 5 | (4.8) | |
More than 10 but less than 20 | 40 | (38.1) | |
More than 20 | 60 | (57.1) | |
Smoking duration | |||
Less than 5 years | 3 | (2.9) | |
More than 5 years but less than 10 years | 10 | (9.5) | |
More than 10 years but less than 15 years | 39 | (37.1) | |
More than 15 years but less than 20 years | 17 | (16.2) | |
More than 20 years but less than 25 years | 25 | (23.8) | |
More than 25 years | 11 | (10.5) | |
Length of smoking abstinence | |||
More than 6 months but less than 1 year | 20 | (19.0) | |
More than 1 year but less than 5 years | 29 | (27.6) | |
More than 5 years but less than 10 years | 30 | (28.6) | |
More than 10 years | 26 | (24.8) | |
Number of previous attempts to quit smoking | |||
None | 46 | (43.8) | |
one | 26 | (24.8) | |
two | 13 | (12.4) | |
three times | 9 | (8.6) | |
4 times | 4 | (3.8) | |
5 times | 4 | (3.8) | |
More than 10 times | 3 | (2.9) | |
(n=105) | ||||||||
|---|---|---|---|---|---|---|---|---|
Mean | SD | Ceiling effect | Floor effect | I-T Correlation | GP Analysis P Value | |||
1 | I had wanted to try to quit smoking for some time | 2.733 | ± | 1.031 | 3.764 | 1.702 | .435 | .000 |
2 | I felt that that stopping smoking would be more beneficial | 3.429 | ± | 0.807 | 4.235 | 2.622 | .443 | .000 |
3 | I was not willing to gradually reduce the number of cigarettes and stop | 2.657 | ± | 1.175 | 3.832 | 1.482 | .421 | .000 |
4 | I always kept in mind that if I smoked, it would be the end of me | 2.448 | ± | 1.201 | 3.648 | 1.247 | .596 | .000 |
5 | Tried to build on my efforts to quit smoking every day | 2.519 | ± | 1.199 | 3.718 | 1.321 | .596 | .000 |
6 | I can't tolerate other people smoking at work | 1.762 | ± | 0.946 | 2.708 | 0.816 | .312 | .001 |
7 | Smoking cessation has improved my reputation among people around me | 2.010 | ± | 0.872 | 2.881 | 1.138 | .351 | .001 |
8 | I didn't have a strong desire to quit smoking* | 2.686 | ± | 1.146 | 3.832 | 1.540 | .319 | .000 |
9 | Going to a smoking area became a hassle | 2.139 | ± | 1.123 | 3.261 | 1.016 | .267 | .001 |
10 | I can now create an environment where I don't have to smoke, such as at home or in my car | 3.067 | ± | 1.085 | 4.152 | 1.981 | .426 | .001 |
11 | I have learned to get through it if I can resist the urge to smoke for a few minutes | 2.779 | ± | 1.140 | 3.919 | 1.639 | .587 | .000 |
12 | Told others I was quitting smoking | 3.029 | ± | 1.113 | 4.142 | 1.915 | .444 | .000 |
13 | Increased involvement with non-smokers | 1.743 | ± | 0.832 | 2.575 | 0.910 | .343 | .008 |
14 | Conscious striving to lose weight | 2.200 | ± | 1.004 | 3.204 | 1.196 | .251 | .013 |
15 | Never thought about quitting smoking for health reasons* | 2.229 | ± | 1.179 | 3.407 | 1.050 | .224 | .046 |
16 | Continued smoking became bothersome | 2.462 | ± | 1.079 | 3.540 | 1.383 | .289 | .018 |
17 | The passage of time seemed longer | 2.029 | ± | 0.965 | 2.994 | 1.063 | .344 | .049 |
18 | I am less likely to feel a strong urge to smoke | 3.429 | ± | 0.864 | 4.293 | 2.564 | .332 | .015 |
19 | When I wanted to smoke, I changed my location and calmed myself down | 1.914 | ± | 0.931 | 2.846 | 0.983 | .463 | .000 |
20 | Better concentration at work | 2.286 | ± | 0.968 | 3.254 | 1.318 | .459 | .000 |
21 | Felt I should have quit smoking cigarettes earlier | 2.533 | ± | 1.057 | 3.590 | 1.477 | .509 | .000 |
22 | I didn't have a clear reason to quit smoking* | 2.490 | ± | 1.269 | 3.760 | 1.221 | -.020 | .626 |
23 | I couldn't get people close to me to approve of my smoking | 1.798 | ± | 0.918 | 2.716 | 0.880 | .287 | .021 |
24 | I failed to quit smoking and didn't want people to point it out to me | 1.923 | ± | 1.040 | 2.963 | 0.883 | .551 | .000 |
25 | I can now perceive taste clearly | 2.362 | ± | 1.030 | 3.392 | 1.332 | .427 | .010 |
26 | When I wanted to smoke, I thought about something other than cigarettes to distract myself | 2.124 | ± | 1.089 | 3.213 | 1.035 | .642 | .000 |
27 | I no longer have to keep people waiting | 2.240 | ± | 1.110 | 3.351 | 1.130 | .456 | .005 |
28 | Proud of the hardest experience of my life | 1.648 | ± | 0.855 | 2.502 | 0.793 | .517 | .000 |
29 | Felt that cigarettes would eventually become unnecessary for me | 2.510 | ± | 1.024 | 3.534 | 1.486 | .417 | .000 |
30 | I expected to be disliked by others in the future | 2.442 | ± | 0.984 | 3.426 | 1.459 | .521 | .000 |
31 | I endured desperately trying to stay free of smoking | 2.269 | ± | 1.054 | 3.323 | 1.215 | .644 | .000 |
32 | Less time frustrated with wanting to smoke | 2.733 | ± | 1.068 | 3.801 | 1.666 | .433 | .000 |
33 | I distracted myself by eating gum or candy | 2.429 | ± | 1.091 | 3.519 | 1.338 | .512 | .000 |
34 | Cigarette-free situation is fresh and good | 2.752 | ± | 1.026 | 3.779 | 1.726 | .599 | .000 |
35 | I don't feel healthier after quitting smoking | 2.529 | ± | 1.052 | 3.580 | 1.477 | .117 | .037 |
36 | The places where I can smoke at work have been reduced | 3.442 | ± | 0.868 | 4.311 | 2.574 | .371 | .004 |
37 | I have several overlapping reasons to quit smoking | 2.924 | ± | 1.062 | 3.986 | 1.861 | .478 | .000 |
38 | I got through it with a strong will to quit smoking | 2.933 | ± | 1.077 | 4.010 | 1.857 | .603 | .000 |
39 | I am no longer distracted by the strong urge to smoke | 3.124 | ± | 0.917 | 4.040 | 2.207 | .486 | .008 |
40 | When I wanted to smoke, I took something to hold me over | 2.133 | ± | 0.991 | 3.124 | 1.142 | .701 | .000 |
41 | Improved physical condition | 2.533 | ± | 0.910 | 3.443 | 1.623 | .496 | .000 |
42 | The social environment has become difficult for smokers | 3.569 | ± | 0.682 | 4.251 | 2.886 | .312 | .001 |
43 | I knew stopping smoking was hard | 2.867 | ± | 1.057 | 3.923 | 1.810 | .628 | .000 |
44 | I didn't smoke because I remembered the painful experience right after I quit smoking | 2.117 | ± | 1.022 | 3.139 | 1.094 | .571 | .000 |
45 | I now have the prospect of continuing being abstinent from smoking | 3.210 | ± | 0.906 | 4.116 | 2.303 | .424 | .003 |
46 | Become stricter on tobacco etiquette | 3.000 | ± | 0.961 | 3.961 | 2.039 | .479 | .000 |
47 | It is a great way to save money. | 1.790 | ± | 0.817 | 2.607 | 0.974 | .440 | .000 |
Entire scale | 118.110 | 21.426 |
Factor | ||||
|---|---|---|---|---|
1 | 2 | 3 | ||
Factor 1 [Status of response to smoking cravings] | ||||
31 | I endured desperately trying to stay free of smoking | .855 | -.055 | .011 |
44 | I didn't smoke because I remembered the painful experience right after I quit smoking | .714 | .020 | -.133 |
26 | When I wanted to smoke, I thought about something other than cigarettes to distract myself | .686 | .207 | -.074 |
43 | I knew stopping smoking was hard | .604 | .022 | .136 |
5 | Tried to build on my efforts to quit smoking every day | .594 | -.254 | .391 |
17 | The passage of time seemed longer | .586 | .142 | -.237 |
4 | I always kept in mind that if I smoked, it would be the end of me | .534 | -.078 | .274 |
32 | Less time frustrated with wanting to smoke | .506 | .099 | -.051 |
40 | When I wanted to smoke, I took something to hold me over | .489 | .223 | .149 |
Factor 2 [Perceived benefits associated with successful smoking cessation] | ||||
20 | Better concentration at work | -.114 | .724 | .061 |
41 | Improved physical condition | .198 | .582 | -.098 |
46 | Become stricter on tobacco etiquette | .078 | .575 | -.117 |
25 | I can now perceive taste clearly | .186 | .518 | -.132 |
34 | Cigarette-free situation is fresh and good | .117 | .498 | .266 |
Factor 3 [Positive perception of smoking cessation] | ||||
8 | I didn't have a strong desire to quit smoking (R) | .068 | -.214 | .622 |
1 | I had wanted to try to quit smoking for some time | -.152 | .092 | .614 |
37 | I have several overlapping reasons to quit smoking | .078 | -.049 | .596 |
21 | Felt I should have quit smoking cigarettes earlier | -.131 | .448 | .488 |
29 | Felt that cigarettes would eventually become unnecessary for me | -.127 | .339 | .434 |
Cronbach's α (full scale) =.876 | ||||
Inter-factor correlations | .873 | .759 | .702 | |
Factor 1 | 1.000 | |||
Factor 2 | .334 | 1.000 | ||
Factor 3 | .515 | .367 | 1.000 | |
Status of response to smoking cravings | |
Q31 | I endured desperately trying to stay free of smoking |
Q44 | I didn't smoke because I remembered the painful experience right after I quit smoking |
Q26 | When I wanted to smoke, I thought about something other than cigarettes to distract myself |
Q43 | I knew stopping smoking was hard |
Q5 | Tried to build on my efforts to quit smoking every day |
Q17 | The passage of time seemed longer |
Q4 | I always kept in mind that if I smoked, it would be the end of me |
Q32 | Less time frustrated with wanting to smoke |
Q40 | When I wanted to smoke, I took something to hold me over |
Perceived benefits associated with successful smoking cessation | |
Q20 | Better concentration at work |
41 | Improved physical condition |
Q46 | Become stricter on tobacco etiquette |
Q25 | I can now perceive taste clearly |
Q34 | Cigarette-free situation is fresh and good |
Positive perception of smoking cessation | |
Q1 | I had wanted to try to quit smoking for some time |
Q21 | Felt I should have quit smoking cigarettes earlier |
Q29 | Felt that cigarettes would eventually become unnecessary for me |
| [1] |
IARC, “IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans Vol. 38 Tobacco Smoking 1986”. Available from:
https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Tobacco-Smoking-1986 [Accessed 26 October 2023]. |
| [2] |
IARC, “IARC Monographs on the Evaluation of the Carcinogenic Risk of Chemicals to Humans Vol. 83 Tobacco Smoking and Involuntary Smoking 2004”. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK316407/pdf/Bookshelf_NBK316407.pdf [Accessed 26 October 2023]. |
| [3] | Secretan, B., Straif, K., Baan, R., Grosse, Y., Ghissassi, F., Bouvard, V., Benbrahim-Tallaa, L., Guha, N., Freeman, C., Galichet, L., Cogliano, V. A review of human carcinogens-Part E: tobacco, areca nut, alcohol, coal smoke, and salted fish. Lancet Oncol. 2009, 10(11), 1033-1034, |
| [4] | Ueshima, K. Tracking research (NIPPON DATA) of fundamental studies on 1980 circulatory diseases. Journal of the Japanese Association for Cerebro-Cardiovascular Disease Control. 1997, 31(3), 231-237, |
| [5] | Mannami, T., Iso, H., Baba, S., Sasaki, S., Okada, K., Konishi, M., Tsugane, S. Cigarette smoking and risk of stroke and its subtypes among middle-aged Japanese men and women: The JPHC study cohort I. Stroke. 2004, 35(6), 1248-1253. |
| [6] | Ishii, Y. Smoking and respiratory diseases. Nihon rinsho. Japanese journal of clinical medicine. 2013, 71(3), 416-420. |
| [7] | Willi, C., Bodenmann, P., Ghali, W, A., Faris, P, D., Cornuz, J,. Active smoking and the risk of type 2 diabetes: a systematic review and meta-analysis. JAMA. 2007, 298(22), 2654-2664. |
| [8] |
Ministry of Health, Labor and Welfare, Outline of the National Health and Nutrition Survey Japan October 2020. Available from:
https://www.mhlw.go.jp/content/10900000/000687163.pdf [Accessed 26 October 2023]. |
| [9] |
World Health Organization, WHO Global Report on Trends in Prevalence of Tobacco Use 2000-2025 Fourth Edition 2021. Available from:
http://apps.who.int/bookorders [Accessed October 26, 2023]. |
| [10] | Hattori, S. Syogai Ningen Hattatsuron Ningeneno fukai rikaito aijyowo hagukumutameni [Lifelong Human Development: To Develop a Deep Understanding and Love for Human Beings]. 3rd Ed. Tokyo: Igaku Shoin; 2020, pp. 133-139. |
| [11] | Funajima, N., Mochizuki, M. Seijinnkino kokorotoshintai [Mind and Body in Adulthood]. Kangonotameno Ningenhattatsugaku [Human Development for Nursing], 5th Ed. Tokyo: Igaku Shoin, 2017, pp. 220-250. |
| [12] |
Ministry of Health, Labor and Welfare, Outline of the Patient Survey Japan 2022. Available from:
https://www.mhlw.go.jp/toukei/saikin/hw/kanja/20/dl/kanjya.pdf [Accessed October 26, 2023]. |
| [13] |
Ministry of Health, Labor and Welfare, Kinen Shien Manyuaru [Smoking Cessation Support Manual] 2006. Available from:
http://www.mhlw.go.jp/topics/tobacco/kin-en-sien/manual/index.html [Accessed October 26, 2023]. |
| [14] |
Ministry of Health, Labor and Welfare, Kinen Shien Manyuaru Dai2ban [Smoking Cessation Support Manual, 2nd Ed] 2013. Available from:
http://www.mhlw.go.jp/topics/tobacco/kin-en-sien/manual2/ [Accessed October 26, 2023]. |
| [15] |
Ministry of Health, Labor and Welfare, The National Health and Nutrition Survey Japan September 2018. Available from:
https://www.mhlw.go.jp/content/10904750/000351576.pdf [Accessed October 26, 2023]. |
| [16] | Nihei, E., Anzai, Y. Study of characteristics of experience in successful smoking cessation among middle-aged male workers in Japan. Sangyo Eiseigaku Zasshi. 2022, 64(4), 173-185. |
| [17] | Hendricks, P, S., Wood, S, B., Hall, S, M. Smokers’ Expectancies for Abstinence: Preliminary Results from Focus Groups. Psychology of Addictive Behaviors. 2009, 23(2), 380-385. |
| [18] | Abrams, K., Zvolensky, M, J., Dorman, L., Gonzalez, A., Mayer, M. Development and validation of the smoking abstinence expectancies questionnaire. Nicotine and Tobacco Research. 2011, 13(12), 1296-1304. |
| [19] | Thomas, D., Mackinnon, A, J., Bonevski, B., Abramson, M, J., Taylor, S., Poole, S, G., Weeks, G., Dooley, M., George, J. Development and validation of a 21-item challenges to stopping smoking (CSS-21) scale. British Medical Journal Open. 2016, 31, 6(3), |
| [20] |
Yoshii, C., Kano, M., Isomura, T., Kunitomo, F., Aizawa, M., Harada, H., Harada, S., Kawanami, Y., Kido, M. An Innovative Questionnaire Examining Dependence, “The Kano rlest fbr Social (KTSND)”. Journal of UOEH. 2006, 28(1), 45-55.
https://www.jstage.jst.go.jp/article/juoeh/28/1/28_KJ00004291026/_pdf |
| [21] | Naoko, I. Improving the Methodological Quality of the Translation and Cultural Adaptation Process for Patient-Reported Outcome Measures. Japanese Association of Behavioral and Cognitive Therapies. 2015, 41(2), 117-125. |
| [22] | Hori, K. Determining the Number of Factors in Exploratory Factor Analysis. Kagawa University economic review. 2005 77(4), 545-580. |
| [23] | Hirai, A. Kyoiku shinrigaku kenkyunotameno deta bunseki nyumon-Riron to gissen karamanabu SPSS katsuyo Houhou [Introduction to Data Analysis for Educational and Psychological Research: SPSS Applications in Theory and Practice]. Tokyo: Tokyosyoseki; 2017, pp. 3-8, 194, 232-233. |
| [24] | Brown, T, A. Confirmatory Factor Analysis for Applied Research. New York: Guilford Press; 2006, pp. 175, 273, 279, 302-304. |
| [25] | Ojio, S. Hajimeteno kyobunsankouzoubunnseki (dai2ban)-Amos niyoru pass kaiseki [Covariance Structure Analysis for Beginners (2nd Edition) - Path Analysis with Amos], 2th Ed. Tokyo: Tokyosyoseki; 2014, pp. 194. |
| [26] | Nakamura, A. A study on the vilification method for construct validity: focusing on discriminant evidence and nomological evidence. Yokohama Keiei Kenkyu [Yokohama Management Research]. 2009, 30(1), 203-219. |
| [27] | Messick, S. Validity of psychological assessment: Validation of inferences from persons’ responses and performances as scientific inquiry into score meaning. American Psychologist. 1995, 50(9), 741-49. |
| [28] | Zhao, H., Yu, J. Kokyaku no yakuwarininshiki oyobi chikakusareta risuku to sabisusettenmanzoku tono kankei [Relationship between Customer Role Perception and Perceived Risk and Service Contact Satisfaction]. In: Abe S, Niikura T Ed. Shohisyakoudoukenkyu no shintenkai [New Developments in Consumer Behavior Research]. Tokyo: Chikurasyobo; 2004, pp. 59-74. |
| [29] | Hatai, S. Developing a structure and measurement scale for the consumer-brand relationship. Consumer Behavior Research. 2004, 10(1,2), 17-41. |
| [30] | Bagozzi, P, R., Yi, Y. On the evaluation of structural equation. J Acad Mark Sci. 1988, 16(1), 74-94. |
| [31] | Fornell, C., Larcker, F, D. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. Journal of Marketing Research. 1981, 18(1), 39-50. |
| [32] | De, Wulf, K., Odekerken-Schröder, G., Iacobucci, D. Investments in consumer relationships: A cross-country and cross-industry exploration. J Mark, 2001, 65(4), 33–50. |
| [33] |
Japanese Law Translation, Industrial Safety and Health. Act No. 71 of 2018. Available from:
https://www.japaneselawtranslation.go.jp/en/laws/view/3440 [Accessed October 26, 2023]. |
| [34] | Suwa, K., Flores, N, M., Yoshikawa, R., Goto, R., Vietri, J., Igarashi, A. Examining the association of smoking with work productivity and associated costs in Japan. Journal of Medical Economics. 2017, 20(9), 938-944. |
| [35] | Christakis, N, A., Fowler, J, H. The Collective Dynamics of Smoking in a Large Social Network. New England Journal of Medicine. 2008, 358(21), 2249-58. |
APA Style
Nihei, E., Anzai, Y. (2024). The Development and Validation of a Scale to Understand Smoking Cessation Efforts Among Middle-Aged Male Workers. European Journal of Preventive Medicine, 12(2), 47-62. https://doi.org/10.11648/j.ejpm.20241202.13
ACS Style
Nihei, E.; Anzai, Y. The Development and Validation of a Scale to Understand Smoking Cessation Efforts Among Middle-Aged Male Workers. Eur. J. Prev. Med. 2024, 12(2), 47-62. doi: 10.11648/j.ejpm.20241202.13
@article{10.11648/j.ejpm.20241202.13,
author = {Emi Nihei and Yukiko Anzai},
title = {The Development and Validation of a Scale to Understand Smoking Cessation Efforts Among Middle-Aged Male Workers
},
journal = {European Journal of Preventive Medicine},
volume = {12},
number = {2},
pages = {47-62},
doi = {10.11648/j.ejpm.20241202.13},
url = {https://doi.org/10.11648/j.ejpm.20241202.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20241202.13},
abstract = {The purpose of this study was to develop and test the reliability and validity of a scale assessing the efforts made by midlife adult male smokers to quit smoking. The draft of the scale, designated the Smoking Cessation Assessment of Progress Scale (SCAPS), was developed a qualitative inductive analysis of the characteristics of successful smoking cessation efforts among midlife adult male workers in a previous study by the authors. The subjects were men in their 30s and 40s who were employed, had quit smoking for at least six months, and who had succeeded in quitting without seeking outpatient smoking cessation treatment. After a preliminary survey, the main survey was conducted. Data was analyzed using the maximum likelihood Promax rotation method. Confirmatory factor analysis was subsequently conducted, resulting in the identification of three factors and 17 items. The factors identified were "response to smoking cravings," "perceived benefits associated with successful smoking cessation," and "positive perception of smoking cessation. Cronbach's alpha coefficients for each subscale ranged from 0.702 to 0.873, which were generally favorable. Construct validity was generally ensured by confirmatory factor analysis and the estimates extracted from the results for each factor. The reliability and validity of SCAPS were generally verified.
},
year = {2024}
}
TY - JOUR T1 - The Development and Validation of a Scale to Understand Smoking Cessation Efforts Among Middle-Aged Male Workers AU - Emi Nihei AU - Yukiko Anzai Y1 - 2024/05/10 PY - 2024 N1 - https://doi.org/10.11648/j.ejpm.20241202.13 DO - 10.11648/j.ejpm.20241202.13 T2 - European Journal of Preventive Medicine JF - European Journal of Preventive Medicine JO - European Journal of Preventive Medicine SP - 47 EP - 62 PB - Science Publishing Group SN - 2330-8230 UR - https://doi.org/10.11648/j.ejpm.20241202.13 AB - The purpose of this study was to develop and test the reliability and validity of a scale assessing the efforts made by midlife adult male smokers to quit smoking. The draft of the scale, designated the Smoking Cessation Assessment of Progress Scale (SCAPS), was developed a qualitative inductive analysis of the characteristics of successful smoking cessation efforts among midlife adult male workers in a previous study by the authors. The subjects were men in their 30s and 40s who were employed, had quit smoking for at least six months, and who had succeeded in quitting without seeking outpatient smoking cessation treatment. After a preliminary survey, the main survey was conducted. Data was analyzed using the maximum likelihood Promax rotation method. Confirmatory factor analysis was subsequently conducted, resulting in the identification of three factors and 17 items. The factors identified were "response to smoking cravings," "perceived benefits associated with successful smoking cessation," and "positive perception of smoking cessation. Cronbach's alpha coefficients for each subscale ranged from 0.702 to 0.873, which were generally favorable. Construct validity was generally ensured by confirmatory factor analysis and the estimates extracted from the results for each factor. The reliability and validity of SCAPS were generally verified. VL - 12 IS - 2 ER -
Faculty of Nursing, Shumei University, Yachiyo City, Chiba, Japan
School of Nursing, Miyagi University, Taiwa Town, Miyagi, Japan